Download Medication Administration Record Sheet Template
Download Medication Administration Record Sheet Template
Incomplete Consumer Information: Failing to fill out the consumer's name can lead to confusion. Each record should clearly identify the individual receiving medication.
Missing Attending Physician Details: Not including the name of the attending physician can hinder communication and accountability. It's important to document who is overseeing the patient's care.
Incorrect Medication Hour: Marking the wrong hour for medication administration can result in improper dosing. Accuracy in timing is essential for the effectiveness of the medication.
Failure to Record Administration: Neglecting to document the administration at the time it occurs can lead to gaps in the medical record. This can affect patient safety and care continuity.
Improper Use of Abbreviations: Using abbreviations incorrectly or failing to define them can create misunderstandings. Clarity is crucial in medical documentation to ensure everyone understands the information presented.
When using the Medication Administration Record Sheet, keep these key points in mind:
What is the purpose of the Medication Administration Record Sheet?
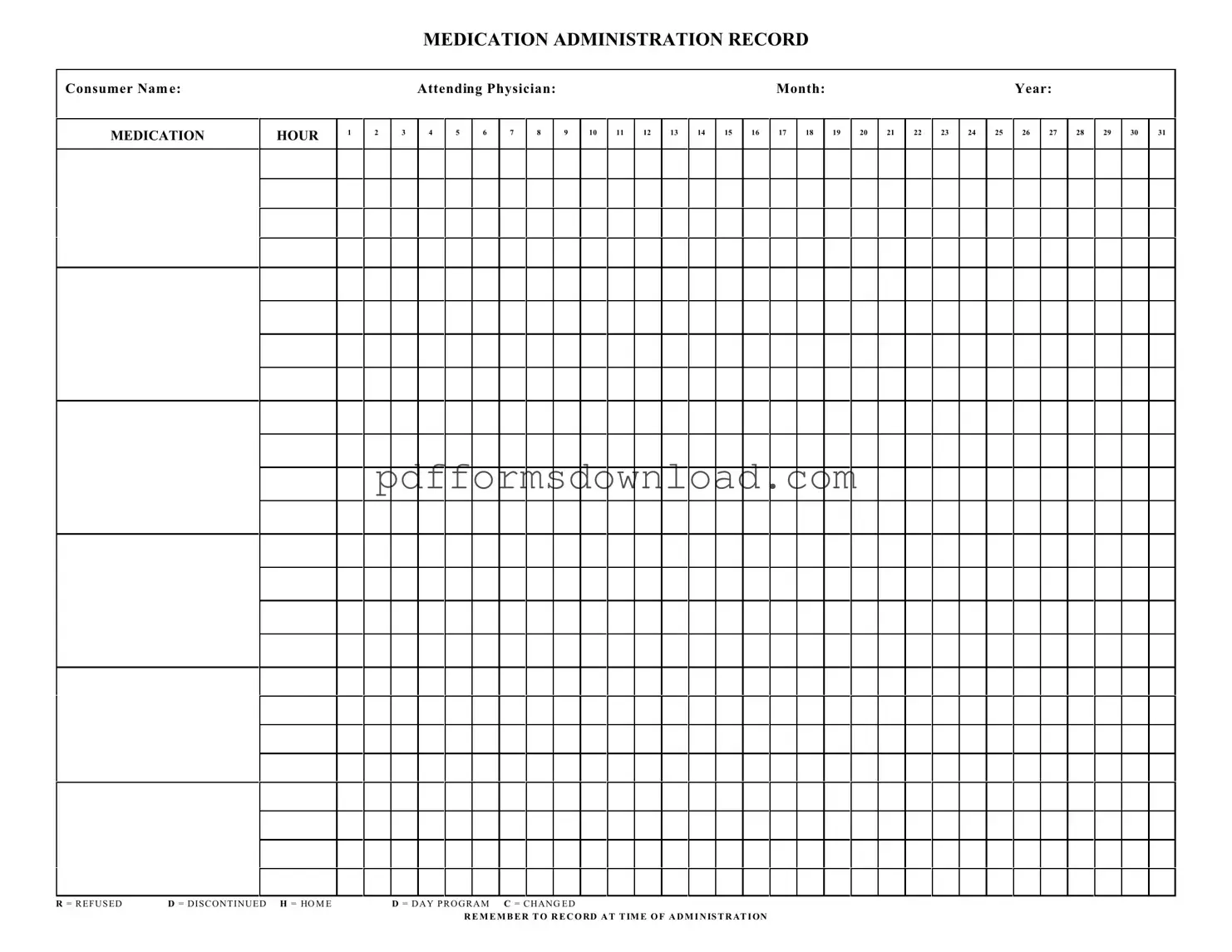
The Medication Administration Record Sheet (MARS) is designed to track and document the administration of medications to consumers. It ensures that medications are given at the correct times and allows healthcare providers to monitor adherence, effectiveness, and any potential side effects.
Who should use the Medication Administration Record Sheet?
This form is intended for use by healthcare professionals, caregivers, and facilities responsible for administering medications to individuals. It is essential for anyone involved in medication management to maintain accurate records for compliance and safety.
What information is required on the Medication Administration Record Sheet?
The MARS requires the consumer's name, the attending physician's name, and the month and year for which the medications are being administered. Additionally, it includes spaces for recording each medication's administration times and any relevant notes regarding refusals or changes in medication.
How do I record medication administration on the form?
When administering medication, mark the appropriate hour on the form. If a medication is refused, discontinued, or changed, use the designated codes: R for refused, D for discontinued, H for home, D for day program, and C for changed. It's crucial to record this information at the time of administration to ensure accuracy.
What should I do if a medication is refused?
If a consumer refuses medication, it must be documented on the MARS by marking the corresponding hour with an "R." Additionally, note any reasons for refusal, as this information is vital for ongoing care and communication with the healthcare team.
Can the Medication Administration Record Sheet be used for multiple consumers?
No, the MARS is specific to individual consumers. Each consumer should have their own record sheet to maintain clear and accurate documentation. This practice helps prevent errors and ensures that each consumer's medication regimen is monitored effectively.
How often should the Medication Administration Record Sheet be updated?
The MARS should be updated daily or whenever medications are administered. Consistent and timely updates are essential for maintaining an accurate record of a consumer's medication history and for ensuring compliance with prescribed treatment plans.
What are the consequences of not properly documenting medication administration?
Failure to document medication administration can lead to serious consequences, including medication errors, adverse health effects, and legal liability. Accurate records are essential for ensuring consumer safety, effective treatment, and compliance with regulatory requirements.
When managing medication for individuals, several important documents work in conjunction with the Medication Administration Record Sheet. Each of these forms plays a vital role in ensuring that medications are administered safely and effectively. Below are some of the commonly used documents alongside the Medication Administration Record Sheet.
These documents, when used together, create a comprehensive system for managing medication administration. They help ensure that patients receive the correct medications safely and that any issues are promptly addressed. By maintaining thorough records, healthcare providers can offer better care and support to those they serve.
High School Transcript - Transcripts are often used for scholarship applications, demonstrating academic merit.
When conducting a transaction involving a mobile home, it is crucial to utilize the Ohio Mobile Home Bill of Sale form, as it serves as a legal instrument to clarify the ownership transfer process. This document not only specifies the necessary details such as the names of the buyer and seller, the mobile home’s specifics, and the agreed sale price but also ensures that both parties are adequately safeguarded. For additional resources and to facilitate the generation of necessary documentation, you can access Ohio PDF Forms.
Death Certificate Affidavit - Removes ambiguity surrounding property rights after a joint tenant’s passing.